ECAIL study protocol published: a new chapter in a decade-long scientific and human journey with the Malin Program
There are major social inequalities in diseases related to diet, physical activity, and sedentary behavior. These energy balance–related behaviors are socially patterned and contribute to a higher prevalence of obesity in disadvantaged groups, starting in early childhood. Beyond financial constraints, these disparities also stem from structural factors (e.g., the availability, accessibility, and affordability of healthy foods) and socio-cultural factors (e.g., social norms and representations).
The Developmental Origins of Health and Disease (DOHaD) paradigm underscores the importance of targeting the first 1,000 days—from pregnancy through the first two years of life—to promote healthy behaviors. However, universal health education campaigns have had limited impact among socially disadvantaged populations, and few early interventions have been adapted and implemented with and for families facing social vulnerability. To promote social equity, such initiatives must go beyond purely information-based approaches and include structural levers, which are essential to strengthen individuals’ agency regarding health behaviors.
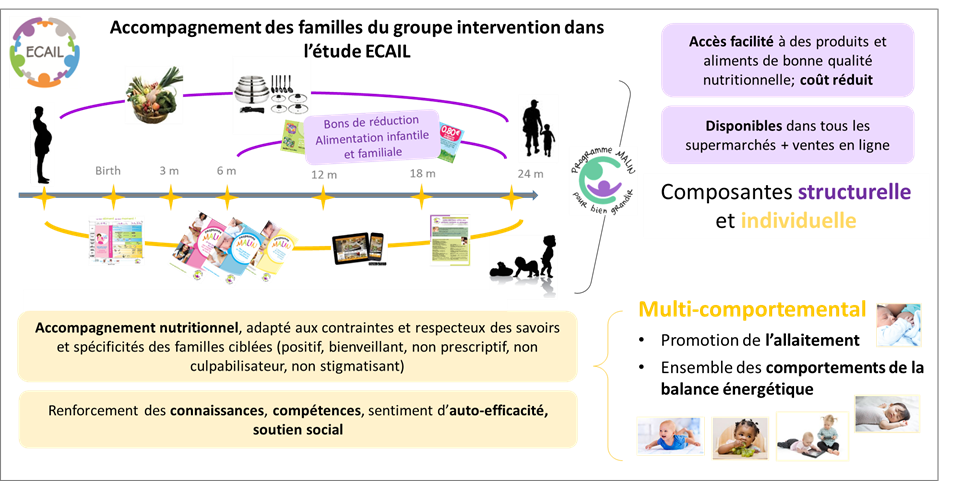
In a context of growing poverty and food insecurity, the ECAIL study aims to evaluate the effectiveness of a multilevel program, called Malin. Co-designed with families and community stakeholders (through participatory approaches), the program supports parents facing financial constraints from pregnancy onward. It combines an educational component (practical advice and tips to support breastfeeding, encourage healthier eating, promote more active lifestyles, and reduce screen time) with non-stigmatizing financial support (discounted fruit and vegetable baskets, affordable kitchen equipment, and vouchers for nutritious foods redeemable in any supermarket).
ECAIL is a randomized controlled trial conducted since 2017 in Lille and Valenciennes, including over 600 pregnant women in socially vulnerable situations, followed at home by dietitians until the child’s second birthday. The intervention group participates in the Malin program, while the control group receives usual care. Quantitative data (medical records, face-to-face questionnaires, anthropometric measurements) and qualitative data (interviews, focus groups) are collected at multiple time points. At the end of trial implementation, planned for 2026, analyses will assess the program’s effects on breastfeeding, complementary feeding, early growth, diet quality, and lifestyle patterns at 12 and 24 months, as well as on the risk of overweight at 24 months.
The process evaluation, at the intersection of epidemiology and social sciences, will help to better understand in which contexts, for whom, and at what intensity the intervention has been most effective, as well as to identify the levers influenced by the program (mechanisms of action) and the barriers encountered. These findings will inform the optimization and progressive scale-up of the Malin program, which already reaches 150,000 socially disadvantaged children and families in France and aims to support twice as many in the coming years.
- Scientific publication: Lioret S, Sion O, Hincker P, Béghin L, de Lauzon-Guillain B, Cavalli B, Salinier C, Turck D, Perez N, Subtil D, Brun S, Charlier M, Creps E, Dehon A, Le Gal C, Poquet D, Sauvegrain P, Heude H, Deplanque D, Meyran D, Devouge P, Ley D, Charles MA. Home visiting intervention over pregnancy and the first two years of life to promote healthy feeding practices and energy balance-related behaviors and prevent obesity risk in children from socially disadvantaged families: protocol for a participant-blinded, two-arm, parallel-group randomized controlled trial—the ECAIL study. BMC Public Health. 2025;25:3659. 2025;25:3659. doi: 10.1186/s12889-025-25004-0
- Home visiting intervention over pregnancy and the first two years of life to promote healthy feeding practices and energy balance-related behaviors and prevent obesity risk in children from socially disadvantaged families: protocol for a participant-blinded, two-arm, parallel-group randomized controlled trial—the ECAIL study – PMC
By Sandrine Lioret